AUCTORES
Globalize your Research

Research Article | DOI: https://doi.org/10.31579/2642-9756/006
School of Health Sciences and Social Works, University of Portsmouth, UK.
*Corresponding Author: Mohammad Mahbubur Rahman
Citation: Mohammad Mahbubur Rahman, and Saseendran Pallikadavath.Direct and Indirect Effects of Janani Suraksha Yojana on Antenatal Care and Institutional Delivery.Doi:10.31579/2642-9756/006
Copyright: © 2019. Mohammad Mahbubur Rahman . This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 30 November -0001 | Accepted: 01 February 2019 | Published: 27 February 2019
Keywords: janani suraksha yojana; demand-side financing; propensity score matching; DLHS; WHO; LPS; HPS
Janani Suraksha Yojana (JSY) provides conditional cash incentives to eligible pregnant women in India so that they can take at least three antenatal care services including tetanus injection and iron-folic acid, to deliver their babies in health institutions, and to take at least one postnatal service for them and their neonatal babies. We examine its effects on antenatal care and the institutional delivery. We also decompose effects into direct and indirect categories, deriving parameters from the theoretical model, then estimating them using several regression methods including the propensity score matching. We use the fourth round of the District Level Household Survey (DLHS), which has an advantage over the previous waves of DLHS.
Every year globally, on average 303,000 women die at the time of pregnancy and childbirth, around 2.7 million babies die within the first 28 days of their life, and stillbirths are approximately 2.6 million (WHO, 2016). Pregnant women's lack of access to quality skilled care before, during and after childbirth, is identified as the main reason for these deaths (WHO, 2017). If uptakes of maternal and child health care services increase, these deaths are expected to reduce significantly.
For many years, by increasing facilities of maternal and child health care services, policymakers were trying to reduce maternal and child mortality. However, day by day, they also realized that an increase in the supply of healthcare facilities, such as medical staff, medicines, and machines, alone cannot increase uptakes of maternal and child health care services at an expected level, especially in a setting where health care facilities are not free, and prices of such facilities are not attainable for more impoverished people (Bhatia et al., 2006; Bhatia and Gorter, 2007; Ensor and Cooper, 2004; Koblinsky et al., 2006; Thaddeus and Maine, 1994).
The success of conditional cash transfer programs (for example, Progressa in Mexico), in the case of human capital and general health in the 1990s, motivated many policymakers of public health. In the spirit of Progressa, since the late 1990s, many developing countries have started conditional cash transfer programs to increase the uptakes of maternal and child health care services (Ensor et al., 2017; Yang et al., 2016; Kuwawenaruwa et al., 2016; Kingkaew et al., 2016; Engineer et al., 2016; Skiles et al., 2015). Such programs are commonly called Demand Side Financing (DSF) program, as they are meant to increase the demand for maternal and child health care services by reducing the relative prices of them (Gertler and Van der Gaag, 1990). Besides the supply side improvement policy, a DSF program has been found useful in increasing the uptakes of desired maternal and child health care services in most of the cases (Anwar et al., 2008, Behrman and Knowles, 1998, Bhatia et al., 2006, Bhatia and Gorter, 2007, Van de Poel et al., 2014).
In the context of high rates of maternal and neonatal death, India launched the world’s largest DSF program, named as Janani Suraksha Yojana (JSY or safe motherhood scheme in English), in 2005. The ultimate goal of JSY is to reduce maternal and neonatal death through increasing the institutional delivery. It covers more than 10 million women a year (MoHFW, 2017) and provides conditional cash transfers to eligible pregnant women so that they can give birth in public or accredited private healthcare facilities, they receive at least three antenatal care (ANC) services including tetanus (TT) injection and iron-folic acid (IFA), and at least one postnatal care (PNC) service for them and their neonatal babies (Yojana, 2006).
A number of studies have previously discussed JSY’s effects on intended and unintended maternal and child health care outcomes (Nandi and Laxminarayan, 2016; Powell-Jackson et al., 2015; Carvalho et al., 2014; Gopalan and Durairaj, 2012; Gupta et al., 2011; Gupta et al., 2012; Lim et al., 2010; Modugu et al., 2012). All of these studies, which focused on institutional delivery, have established high positive effects of JSY on institutional delivery. However, findings of the effects of JSY on ANC and PNC are varied, as statistically insignificant effects have also been found on these intended outcomes (Powell-Jackson et al., 2015). On the other hand, significant effects have been found on some unintended outcomes (Powell-Jackson et al., 2015). For example, JSY significantly increases the probability of pregnancy, and JSY women start breastfeeding their neonatal babies earlier than non-JSY women.
Previous prominent studies (Nandi and Laxminarayan, 2016; Powell-Jackson et al., 2015; Carvalho et al., 2014; Lim et al., 2010) used data from second and third rounds of a repeated cross-section, District Level Household Survey (DLHS), surveyed in 2002-2004 and 2007-2008 respectively. The second round was surveyed before JSY, and the third round was surveyed when JSY was in its early stages when many women were not aware of it. There is a potential for the selection bias in that early round. The chance is high because JSY’s operation has been running since 2007 (Das et al., 2011). Additionally, many women responded as JSY beneficiaries when they were not (Das et al., 2011). This implies that the treatment group included control women. Because of this and the possible selection bias, previous results are likely to have substantial downward biases.
We use the fourth round of DLHS (DLHS-4), which was surveyed in 2013-2014 when JSY was a mature program. It is unlikely that DLHS-4 has such extensive problems. We expect statistically significant effects on all intended outcomes. However, the objective of our paper is not only estimating JSY’s effects on the intended outcomes but also to decompose those effects into the direct and indirect effects. There is no doubt that being a part of JSY’s cash incentive an intended outcome can be affected by JSY directly. JSY can also affect it indirectly by changing another intended outcome if two outcomes are connected. We shall capture here both direct and indirect effects on the intended outcomes, and shall see which effects are stronger than the others. We do attempt these decompositions because policymakers will understand how JSY affects the intended outcomes, and then they will be able to take necessary actions to improve them further, and even they may save money to get the same anticipated effects. For example, if JSY works only to increase the utilization of an ANC service, and the utilization of institutional delivery service increases due to the increase in the utilization of an ANC service, JSY may not require to provide extra cash incentives to increase the utilization of institutional delivery service.
In this study, we consider two main intended outcomes – ANC and institutional delivery. We assume that both are connected, and in addition to the direct effect, JSY may have an indirect impact on each through each other. To capture both direct and indirect effects, we initially derive mathematical equations from raw differentials and then develop econometric models to estimate parameters in mathematical equations.
After this introductory section, we briefly discuss the program, JSY, in Section II. Section III formulates both theoretical and econometric models. Section IV describes data, and Section V presents results. Finally, Section VI contains the discussion and conclusion of the study.
India is steadily improving concerning reducing maternal and child mortality (Tandon, 2016; Registrar General of India, 2013). In spite of the steady progress, it still suffers from the highest under-five child mortality rate in the world (Tandon, 2016). The number of maternal deaths in India is higher than such amounts in its close competitors such as Indonesia and Malaysia (UNICEF, 2017). Moreover, the national figures hide the situation at the state level. In general, the northern states have very high maternal and child mortality rates in comparison to the southern states (Registrar General of India, 2013).
In the above setting, on 12th April 2005, the world’s largest DSF program, JSY, was launched under the National Rural Health Mission (NRHM) by the prime minister of India. The primary objective of JSY is to increase the institutional delivery, but the ultimate goal of it is reducing maternal and neonatal mortality through increasing the institutional delivery. Along with the financial support of expanding the institutional delivery, JSY also gives financial incentives to increase the uptakes of at least three ANC services including a TT injection and IFA, and at least one PNC service for a mother and her child.
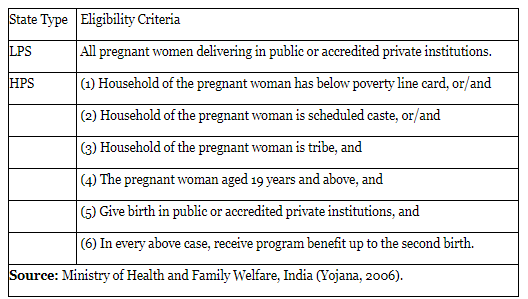
JSY is a universal program in 10 Low Performing States (LPS) – Uttar Pradesh, Uttaranchal, Bihar, Jharkhand, Madhya Pradesh, Chhattisgarh, Assam, Rajasthan, Orissa, and Jammu and Kashmir – where the rates of institutional delivery are very low. In LPS, every pregnant woman who wants to deliver her child in a public or an accredited private hospital is eligible for JSY cash incentives. In other states, which are called High Performing States (HPS), the program gives financial incentives to only socio-economically disadvantaged women. Table (1) lists all eligibility criteria by state type. First, three criteria in HPS are the key criteria which determine whether a woman falls into the socio-economically disadvantaged group. A woman will be selected for JSY if she fulfills any one or all criteria in addition to fulfilling the other criteria. Criteria (4) and (6) in HPS are set to discourage baby boom, and (5) is a cost-effective criterion. It should be noted that the age criterion has been withdrawn recently. However, at the time of our data, the criterion remained and so was kept in this study.
There are many field workers in the program who are appointed to work as intermediaries between the program administrators and the pregnant women. A field worker is called an accredited social health activist (ASHA). ASHAs identify the eligible pregnant women for JSY, and they help them from birth registration to the PNC service. They also prompt women to use the institutional delivery service. An ASHA receives cash incentives for his/her activities. Table 2 provides the information of cash incentives of JSY (in Indian Rupees) for both an eligible woman and an ASHA. LPS mothers receive a higher amount of cash than HPS mothers, in both rural and urban areas. ASHA’s cash incentives do not vary by state type but vary by rural and urban areas. For both mothers and ASHAs, cash incentives are higher in the rural area than that in the urban area. This is probably the reason that the more destitute women live in the rural area, and rural transportation is costly.
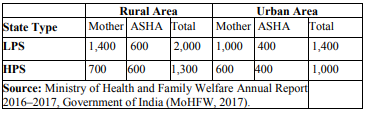
An eligible pregnant woman aiming to deliver her baby in the public health institute receives her entire cash entitlement in one go at the health institution. An accredited private health institute reimburses the thirdfourth of the cash incentive in the first visit of an eligible woman who aims to deliver her baby there. A qualified woman also receives at least 250 rupees for transportation costs, which may vary by location and state. Up to an additional 1,500 rupees is given to her in the case of the caesarian section or obstetric complications. If she wants to deliver at home, she only receives 500 rupees. An ASHA’s cash payment is made in two installments. The first part of the payment is given when he/she goes to the health institute with the pregnant women for the first time, and the second part of the payment is given after the PNC services taken by a mother.
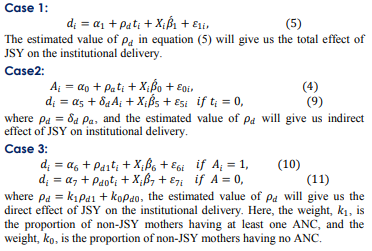
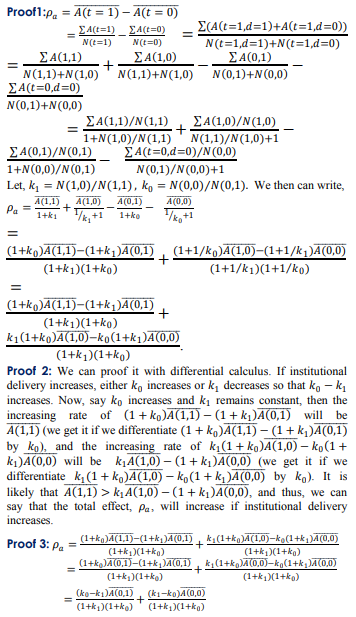
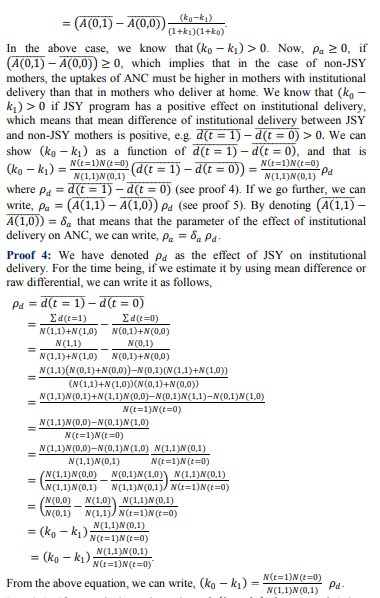
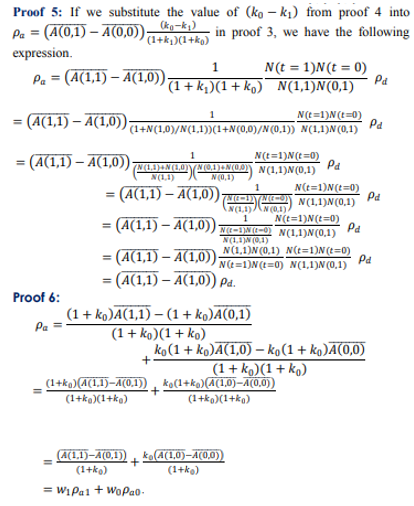
A. Mathematical Models

Case 2: The effect of JSY on ANC, when JSY has no direct effect on ANC, but has a direct effect on the institutional delivery. We can now show that
Data from the fourth round of the District Level Household Survey (DLHS-4) was used, which was surveyed in 2013-14. Because of surveying different households in different waves, DLHS is considered as a repeated cross-section. We do not use other previous waves of it. DLHS-1 and DLHS-2 were surveyed before the implementation of JSY, and DLHS-3 was surveyed immediately after the implementation of JSY. DLHS-3 misclassified many non-JSY beneficiaries as JSY beneficiaries (Das et al., 2011) and therefore, it is likely to produce biased results. DLHS-4 collected data from 378,487 households located in 18 highperforming states and 3 high performing territories. However, for the data on the maternal and child health care, the latest wave surveyed only 86,000 women who gave their last births from 2008. The information about maternal and child health care was collected from only their last births. So, the times of all last births surveyed by DLHS-4 fell within the period of JSY’s proper implementation (2007- present). Therefore, as opposed to DLHS-3, DLHS-4 has a less chance of misclassifying untreated women as treated. Among 86,000 women, about 22% responded as JSY beneficiaries, and about 4% were the beneficiaries of other schemes.
We dropped other schemes’ recipients from our data, as the study’s focus is JSY’s evaluation. Besides, they may make our results biased, as those schemes might have different cash incentives. In this way, a significant amount of data has been dropped. Moreover, many women have been dropped automatically from the data, as they did not respond to the questions on variables used in this study (e.g., missing value problem). In Table 3, we present means of both outcome variables (A and d) and covariates by the JSY treatment status (t). It should be noted that covariates include both the program eligibility criteria such as poverty dummy, scheduled caste dummy, and tribe dummy and the self-selection criteria such as wealth index, age, education, religion, and residence. Among these covariates, education and age are individual characteristics, and all others are women’s household characteristics. Other than wealth index, all variables are generated in straight away from the data. Using the principal component analysis, wealth index is generated from the availability of a household’s assets, which include cooking fuel, house type, number of dwelling rooms, electricity, house ownership, landholding, radio, television, computer, internet, telephone, mobile phone, washing machine, refrigerator, sewing machine, watch, bicycle, motorcycle, car, tractor, tube well, cart and air cooler.

However, Table 3 also presents the number of observations with each mean. Differences of means between JSY and non-JSY women are also shown with their p values. Combining JSY and non-JSY women, there are around 73,000 women in most of the cases. Among them, around 22% are treated by JSY. We see that almost all variables have significantly different means between JSY and non-JSY women, as p values are approximately zero. We expect such results in the case of
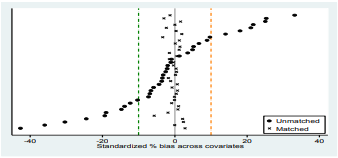
Note: Data are from DLHS-4. Biases of covariates give a better indication of the randomization than means differences of covariates. In a bias calculation, a mean difference of a covariate between the treatment and control group is standardized by the standard errors. Bias calculation is slightly different for a continuous covariate and a dummy covariate (Thomas, 2003). Say,
For three different cases, we estimate the effects of JSY on ANC and the institutional delivery. As we know, the first case shows the overall effects, the second case shows the indirect effects, and the third case shows the direct effects.
For comparisons, in every case, we run linear probability models (OLS regressions) and logit regressions in addition to the PSM regressions and raw estimates. To maintain the overlapping assumption, we also run PSM regressions for subsamples identified when the propensity score is between 0.10 and 0.90 (Crump et al.; 2009). Thus, PSM with overlapping produces the most reliable estimates here. In the case of PSM, we use the default options in Stata’s psmatch2 command meaning that we run the nearest neighbor PSM.
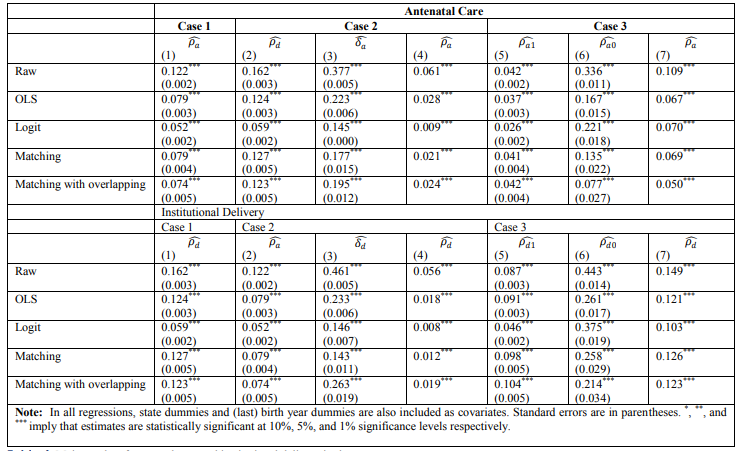
In Table 4, we show the values of the key parameters , which are estimated using equations (2-11). In the first panel (under ANC), (ρ_a ) ̂ in case 1, (ρ_d ) ̂and (δ_a ) ̂in case 2, and (ρ_a1 ) ̂and (ρ_a0 ) ̂in case 3 are estimated from regressions of equations (4-8), which are run using the regression methods mentioned above . Similarly, in the second panel (under institutional delivery ), (ρ_d ) ̂in case 1, (ρ_a ) ̂ and (δ_d ) ̂in case 2, and (ρ_d1 ) ̂and (ρ_d0 ) ̂in case 3 are estimated from regressions of equations (4, 5, 9-11) which are run using those regression methods. All regressions have used covariates listed in Table 3 plus state dummies and birth year dummies. Standard errors of those parameters estimated from regressions are reported in parentheses. All other parameters are estimated without regressions but following equations (2) and (3), and therefore , they do not have any standard errors . For example , (ρ_a ) ̂ in case 2 under ANC is estimated using equation (2). This is a measure of indirect effects of JSY on ANC. (ρ_a ) ̂in case 3 under ANC is estimated using equation (3). This is a measure of the direct effects of JSY on ANC . Similarly, (ρ_d ) ̂ in case 2 under institutional delivery is estimated following equation (2) (meaning similar to equation (2)). This is a measure of indirect effects of JSY on the institutional delivery . (ρ_d ) ̂ in case 3 under institutional delivery is estimated following equation (3) (that means as the similar way of equation (3)). This is a measure of the direct effects of JSY on the institutional delivery. Each regression type shows that the direct effects of JSY are stronger than the indirect effects, in both ANC and institutional delivery.
JSY provides cash incentives to eligible pregnant women to increase both ANC and the institutional delivery. Both of these maternal outcomes are under the continuum of maternal care, and therefore, they are connected with each other. JSY effects each indirectly through the other. If their connections become stronger, the indirect effects will be stronger. Indirect effects also depend on the direct effects of JSY. If we see the numbers in the case of PSM with overlapping in column (3) of Table 4, we understand that the effect of ANC on the institutional delivery is stronger than the reverse effect. The direct effect of JSY on the institutional delivery is much stronger than the direct effect of JSY on ANC (see column (7) of Table (4)). Therefore, the overall effect of JSY on the institutional delivery is much stronger than the overall effect of JSY on ANC (see columns (1) and (2) in Table (4)). Correspondingly, the indirect effect of JSY on the institutional delivery is weaker than the indirect effect of JSY on ANC (see column (4) of Table (4)), in spite of a higher effect of ANC on the institutional delivery than the reverse effect. From a policy perspective, we can say that policymakers should work first to increase the uptake of ANC, and then the institutional delivery will automatically increase as a result of their connections. In Table (3), we can see that the uptake of ANC is 0.949 or 94.9% amongst the JSY women. In other words, we can say that 5.1% of JSY women do not take any ANC service. Policymakers should identify why some of JSY women do not take any ANC service, in spite of cash incentives they receive If cash incentives are insufficient for them, that should be increased so that the uptake of ANC becomes 100%. When women go to health institutions for any ANC service, health professionals should strongly recommend them to have the institutional delivery. In this way, the effect of ANC on the institutional delivery will increase, and thus, the indirect effect and then the overall effect of JSY on the institutional delivery will increase. Policymakers should also identify why 6.5% of JSY women do not go to health institutions for the institutional delivery (see Table (3)). The uptake of the institutional delivery among JSY women should be 100% too, as it is the JSY’s main objective. In this paper, we decompose the effects of JSY on ANC and the institutional delivery. In addition to the methodological contribution, we consider this as an important contribution. After this decomposition, policymakers will now understand how JSY affects ANC and the institutional delivery and how much efforts should be taken to improve them.
Funding: This study was funded by Medical Research Council (MRC), UK (grant number MR/N006267/1).
Conflict of Interest: The authors declare that they have no conflict of interest.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.

Journal of Clinical Cardiology and Cardiovascular Intervention The submission and review process was adequate. However I think that the publication total value should have been enlightened in early fases. Thank you for all.

Journal of Women Health Care and Issues By the present mail, I want to say thank to you and tour colleagues for facilitating my published article. Specially thank you for the peer review process, support from the editorial office. I appreciate positively the quality of your journal.

Journal of Clinical Research and Reports I would be very delighted to submit my testimonial regarding the reviewer board and the editorial office. The reviewer board were accurate and helpful regarding any modifications for my manuscript. And the editorial office were very helpful and supportive in contacting and monitoring with any update and offering help. It was my pleasure to contribute with your promising Journal and I am looking forward for more collaboration.

We would like to thank the Journal of Thoracic Disease and Cardiothoracic Surgery because of the services they provided us for our articles. The peer-review process was done in a very excellent time manner, and the opinions of the reviewers helped us to improve our manuscript further. The editorial office had an outstanding correspondence with us and guided us in many ways. During a hard time of the pandemic that is affecting every one of us tremendously, the editorial office helped us make everything easier for publishing scientific work. Hope for a more scientific relationship with your Journal.

The peer-review process which consisted high quality queries on the paper. I did answer six reviewers’ questions and comments before the paper was accepted. The support from the editorial office is excellent.

Journal of Neuroscience and Neurological Surgery. I had the experience of publishing a research article recently. The whole process was simple from submission to publication. The reviewers made specific and valuable recommendations and corrections that improved the quality of my publication. I strongly recommend this Journal.

Dr. Katarzyna Byczkowska My testimonial covering: "The peer review process is quick and effective. The support from the editorial office is very professional and friendly. Quality of the Clinical Cardiology and Cardiovascular Interventions is scientific and publishes ground-breaking research on cardiology that is useful for other professionals in the field.

Thank you most sincerely, with regard to the support you have given in relation to the reviewing process and the processing of my article entitled "Large Cell Neuroendocrine Carcinoma of The Prostate Gland: A Review and Update" for publication in your esteemed Journal, Journal of Cancer Research and Cellular Therapeutics". The editorial team has been very supportive.

Testimony of Journal of Clinical Otorhinolaryngology: work with your Reviews has been a educational and constructive experience. The editorial office were very helpful and supportive. It was a pleasure to contribute to your Journal.

Dr. Bernard Terkimbi Utoo, I am happy to publish my scientific work in Journal of Women Health Care and Issues (JWHCI). The manuscript submission was seamless and peer review process was top notch. I was amazed that 4 reviewers worked on the manuscript which made it a highly technical, standard and excellent quality paper. I appreciate the format and consideration for the APC as well as the speed of publication. It is my pleasure to continue with this scientific relationship with the esteem JWHCI.

This is an acknowledgment for peer reviewers, editorial board of Journal of Clinical Research and Reports. They show a lot of consideration for us as publishers for our research article “Evaluation of the different factors associated with side effects of COVID-19 vaccination on medical students, Mutah university, Al-Karak, Jordan”, in a very professional and easy way. This journal is one of outstanding medical journal.

Dear Hao Jiang, to Journal of Nutrition and Food Processing We greatly appreciate the efficient, professional and rapid processing of our paper by your team. If there is anything else we should do, please do not hesitate to let us know. On behalf of my co-authors, we would like to express our great appreciation to editor and reviewers.

As an author who has recently published in the journal "Brain and Neurological Disorders". I am delighted to provide a testimonial on the peer review process, editorial office support, and the overall quality of the journal. The peer review process at Brain and Neurological Disorders is rigorous and meticulous, ensuring that only high-quality, evidence-based research is published. The reviewers are experts in their fields, and their comments and suggestions were constructive and helped improve the quality of my manuscript. The review process was timely and efficient, with clear communication from the editorial office at each stage. The support from the editorial office was exceptional throughout the entire process. The editorial staff was responsive, professional, and always willing to help. They provided valuable guidance on formatting, structure, and ethical considerations, making the submission process seamless. Moreover, they kept me informed about the status of my manuscript and provided timely updates, which made the process less stressful. The journal Brain and Neurological Disorders is of the highest quality, with a strong focus on publishing cutting-edge research in the field of neurology. The articles published in this journal are well-researched, rigorously peer-reviewed, and written by experts in the field. The journal maintains high standards, ensuring that readers are provided with the most up-to-date and reliable information on brain and neurological disorders. In conclusion, I had a wonderful experience publishing in Brain and Neurological Disorders. The peer review process was thorough, the editorial office provided exceptional support, and the journal's quality is second to none. I would highly recommend this journal to any researcher working in the field of neurology and brain disorders.
Dear Agrippa Hilda, Journal of Neuroscience and Neurological Surgery, Editorial Coordinator, I trust this message finds you well. I want to extend my appreciation for considering my article for publication in your esteemed journal. I am pleased to provide a testimonial regarding the peer review process and the support received from your editorial office. The peer review process for my paper was carried out in a highly professional and thorough manner. The feedback and comments provided by the authors were constructive and very useful in improving the quality of the manuscript. This rigorous assessment process undoubtedly contributes to the high standards maintained by your journal.

International Journal of Clinical Case Reports and Reviews. I strongly recommend to consider submitting your work to this high-quality journal. The support and availability of the Editorial staff is outstanding and the review process was both efficient and rigorous.

Thank you very much for publishing my Research Article titled “Comparing Treatment Outcome Of Allergic Rhinitis Patients After Using Fluticasone Nasal Spray And Nasal Douching" in the Journal of Clinical Otorhinolaryngology. As Medical Professionals we are immensely benefited from study of various informative Articles and Papers published in this high quality Journal. I look forward to enriching my knowledge by regular study of the Journal and contribute my future work in the field of ENT through the Journal for use by the medical fraternity. The support from the Editorial office was excellent and very prompt. I also welcome the comments received from the readers of my Research Article.

Dear Erica Kelsey, Editorial Coordinator of Cancer Research and Cellular Therapeutics Our team is very satisfied with the processing of our paper by your journal. That was fast, efficient, rigorous, but without unnecessary complications. We appreciated the very short time between the submission of the paper and its publication on line on your site.

I am very glad to say that the peer review process is very successful and fast and support from the Editorial Office. Therefore, I would like to continue our scientific relationship for a long time. And I especially thank you for your kindly attention towards my article. Have a good day!

"We recently published an article entitled “Influence of beta-Cyclodextrins upon the Degradation of Carbofuran Derivatives under Alkaline Conditions" in the Journal of “Pesticides and Biofertilizers” to show that the cyclodextrins protect the carbamates increasing their half-life time in the presence of basic conditions This will be very helpful to understand carbofuran behaviour in the analytical, agro-environmental and food areas. We greatly appreciated the interaction with the editor and the editorial team; we were particularly well accompanied during the course of the revision process, since all various steps towards publication were short and without delay".

I would like to express my gratitude towards you process of article review and submission. I found this to be very fair and expedient. Your follow up has been excellent. I have many publications in national and international journal and your process has been one of the best so far. Keep up the great work.

We are grateful for this opportunity to provide a glowing recommendation to the Journal of Psychiatry and Psychotherapy. We found that the editorial team were very supportive, helpful, kept us abreast of timelines and over all very professional in nature. The peer review process was rigorous, efficient and constructive that really enhanced our article submission. The experience with this journal remains one of our best ever and we look forward to providing future submissions in the near future.

I am very pleased to serve as EBM of the journal, I hope many years of my experience in stem cells can help the journal from one way or another. As we know, stem cells hold great potential for regenerative medicine, which are mostly used to promote the repair response of diseased, dysfunctional or injured tissue using stem cells or their derivatives. I think Stem Cell Research and Therapeutics International is a great platform to publish and share the understanding towards the biology and translational or clinical application of stem cells.

I would like to give my testimony in the support I have got by the peer review process and to support the editorial office where they were of asset to support young author like me to be encouraged to publish their work in your respected journal and globalize and share knowledge across the globe. I really give my great gratitude to your journal and the peer review including the editorial office.

I am delighted to publish our manuscript entitled "A Perspective on Cocaine Induced Stroke - Its Mechanisms and Management" in the Journal of Neuroscience and Neurological Surgery. The peer review process, support from the editorial office, and quality of the journal are excellent. The manuscripts published are of high quality and of excellent scientific value. I recommend this journal very much to colleagues.

Dr.Tania Muñoz, My experience as researcher and author of a review article in The Journal Clinical Cardiology and Interventions has been very enriching and stimulating. The editorial team is excellent, performs its work with absolute responsibility and delivery. They are proactive, dynamic and receptive to all proposals. Supporting at all times the vast universe of authors who choose them as an option for publication. The team of review specialists, members of the editorial board, are brilliant professionals, with remarkable performance in medical research and scientific methodology. Together they form a frontline team that consolidates the JCCI as a magnificent option for the publication and review of high-level medical articles and broad collective interest. I am honored to be able to share my review article and open to receive all your comments.

“The peer review process of JPMHC is quick and effective. Authors are benefited by good and professional reviewers with huge experience in the field of psychology and mental health. The support from the editorial office is very professional. People to contact to are friendly and happy to help and assist any query authors might have. Quality of the Journal is scientific and publishes ground-breaking research on mental health that is useful for other professionals in the field”.

Dear editorial department: On behalf of our team, I hereby certify the reliability and superiority of the International Journal of Clinical Case Reports and Reviews in the peer review process, editorial support, and journal quality. Firstly, the peer review process of the International Journal of Clinical Case Reports and Reviews is rigorous, fair, transparent, fast, and of high quality. The editorial department invites experts from relevant fields as anonymous reviewers to review all submitted manuscripts. These experts have rich academic backgrounds and experience, and can accurately evaluate the academic quality, originality, and suitability of manuscripts. The editorial department is committed to ensuring the rigor of the peer review process, while also making every effort to ensure a fast review cycle to meet the needs of authors and the academic community. Secondly, the editorial team of the International Journal of Clinical Case Reports and Reviews is composed of a group of senior scholars and professionals with rich experience and professional knowledge in related fields. The editorial department is committed to assisting authors in improving their manuscripts, ensuring their academic accuracy, clarity, and completeness. Editors actively collaborate with authors, providing useful suggestions and feedback to promote the improvement and development of the manuscript. We believe that the support of the editorial department is one of the key factors in ensuring the quality of the journal. Finally, the International Journal of Clinical Case Reports and Reviews is renowned for its high- quality articles and strict academic standards. The editorial department is committed to publishing innovative and academically valuable research results to promote the development and progress of related fields. The International Journal of Clinical Case Reports and Reviews is reasonably priced and ensures excellent service and quality ratio, allowing authors to obtain high-level academic publishing opportunities in an affordable manner. I hereby solemnly declare that the International Journal of Clinical Case Reports and Reviews has a high level of credibility and superiority in terms of peer review process, editorial support, reasonable fees, and journal quality. Sincerely, Rui Tao.

Clinical Cardiology and Cardiovascular Interventions I testity the covering of the peer review process, support from the editorial office, and quality of the journal.
